2019-InceptionGCN, Receptive Field Aware Graph-基于矩阵+图表示-rrr1
需积分: 0 64 浏览量
2022-08-04
12:25:19
上传
评论
收藏 656KB PDF 举报


InceptionGCN: Receptive Field Aware Graph
Convolutional Network for Disease Prediction
Anees Kazi
1
, Shayan Shekarforoush
2
, S.Arvind krishna
3
, Hendrik Burwinkel
1
,
Gerome Vivar
1,4
, Karsten Kort
¨
um
5
, Seyed-Ahmad Ahmadi
4
, Shadi
Albarqouni
1
, and Nassir Navab
1,6
1
Computer Aided Medical Procedures (CAMP), Technical University of Munich,
Munich, Germany
2
Sharif University of Technology, Tehran, Iran
3
Department of Computer Science and Engineering, National Institute of Technology
Tiruchirappalli, India
4
German Center for Vertigo and Balance Disorders, Ludwig Maximilians Universit
¨
at
M
¨
unchen, Germany
5
Augenklinik der Universit
¨
at, Klinikum der Universit
¨
at M
¨
unchen, Germany
6
Whiting School of Engineering, Johns Hopkins University, Baltimore, USA
Abstract. Geometric deep learning provides a principled and versatile
manner for integration of imaging and non-imaging modalities in the
medical domain. Graph Convolutional Networks (GCNs) in particular
have been explored on a wide variety of problems such as disease pre-
diction, segmentation, and matrix completion by leveraging large, multi-
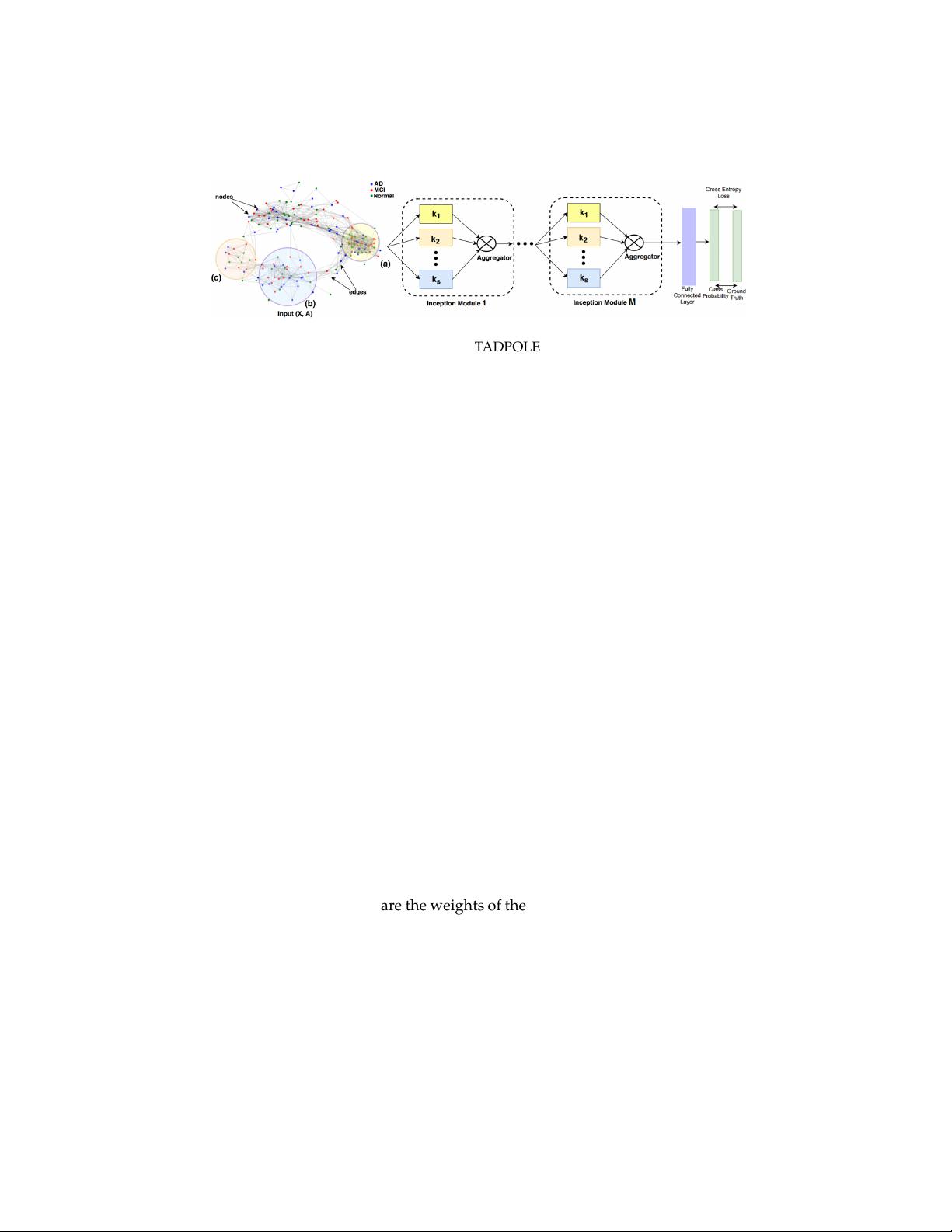
modal datasets. In this paper, we introduce a new spectral domain archi-
tecture for deep learning on graphs for disease prediction. The novelty lies
in defining geometric ’inception modules’ which are capable of captur-
ing intra- and inter-graph structural heterogeneity during convolutions.
We design filters with different kernel sizes to build our architecture. We
show our disease prediction results on two publicly available datasets.
Further, we provide insights on the behaviour of regular GCNs and our
proposed model under varying input scenarios on simulated data.
1 Introduction
There is an increasing focus on applying deep learning on unstructured data in
the medical domain, especially using Graph Convolutional Networks (GCNs)
[1]. Multiple applications have been demonstrated so far, including Autism
Spectrum Disorder prediction with manifold learning to distinguish between
diseased and healthy brains [2], matrix completion to predict the missing val-
ues in medical data [3], and finding drug similarity using graph auto encoders
[4]. In this paper, we study the task of Alzheimer and Autism disease prediction
with complementary imaging and non-imaging multi-modal data.
In above works, GCNs had a remarkable impact on the usage of multi-
modal medical data. One key difference to previous learning-based methods
is to set patients in relation to each other with a neighborhood graph, often by
arXiv:1903.04233v1 [cs.LG] 11 Mar 2019

剩余11页未读,继续阅读













评论0